Clinical Protocols for Optimizing the Ketamine Neuroplasticity Window in TRD (Treatment Resistant Depression)
The landscape of modern neuropsychiatry is undergoing a profound paradigm shift. For decades, the dominant framework for treating Major Depressive Disorder (MDD) and Treatment-Resistant Depression (TRD) relied almost exclusively on the monoaminergic hypothesis. Traditional pharmacotherapies—such as Selective Serotonin Reuptake Inhibitors (SSRIs) and Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)—attempt to increase ambient monoamine concentrations within the synaptic cleft. However, these conventional interventions are fundamentally limited by substantial systemic delays, often requiring weeks or months to demonstrate clinical efficacy, while yielding discouragingly low remission rates for severely afflicted populations.
The introduction of subanesthetic ketamine infusions has completely disrupted this conventional protocol. Ketamine functions not as a slow-acting monoaminergic modifier, but as a rapid-acting glutamatergic modulator capable of inducing robust structural and functional changes in neural architecture within hours. Yet, as clinical adoption expands globally, an urgent consensus has emerged among neuroscientists and clinical strategists: the profound, rapid anti-depressive effects of ketamine are fundamentally baseline alterations that degrade over time if left unsupported. To translate transient symptomatic relief into permanent, structural psychological recovery, medical practices must deploy structured, evidence-based clinical protocols for optimizing the ketamine neuroplasticity window in treatment resistant depression.
The Molecular Cascades of Ketamine Neuroplasticity
To fully understand the clinical necessity of a structured timeline intervention, one must examine the precise molecular mechanisms governing ketamine neuroplasticity. Chronic, unremitting stress and prolonged depressive states inflict severe structural damage upon key regions of the central nervous system, most notably the prefrontal cortex (PFC) and the hippocampus. Under sustained hypercortisolemia, dendritic spines undergo significant atrophy, synaptic density decreases, and functional connectivity across critical neural networks breaks down. This structural regression manifests behaviorally as cognitive rigidity, deep psychological distress, and the persistent ruminative cycles characteristic of TRD.
Ketamine reverses this structural degradation via a sophisticated multi-tier cellular signaling pathway. Operating primarily as a non-competitive antagonist of the N-methyl-D-aspartate (NMDA) receptor, ketamine preferentially blocks NMDA receptors located on inhibitory gamma-aminobutyric acid (GABA)-ergic interneurons. This transient blockade causes a immediate phenomenological reduction in GABA release, effectively removing the biological “brakes” on glutamatergic neurotransmission. The resulting downstream phenomenon is an acute, concentrated surge of presynaptic glutamate within the medial prefrontal cortex.
This localized glutamate surge rapidly targets and activates post-synaptic alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors. The concurrent depolarization of the post-synaptic membrane triggers a voltage-dependent influx of calcium ions, stimulating the rapid exocytosis of endogenous Brain-Derived Neurotrophic Factor (BDNF). BDNF serves as the primary biological catalyst for structural growth, binding directly to tropomyosin receptor kinase B (TrkB) receptors.
This binding event serves as the critical trigger for robust upstream signaling, culminating in immediate mTOR pathway activation ketamine (mammalian target of rapamycin complex 1, or mTORC1). The activation of the mTORC1 pathway functions as the master switch for intra-cellular protein synthesis. It accelerates the localized translation of vital structural proteins, including postsynaptic density protein 95 (PSD-95) and gluR1 AMPA receptor subunits, which are mandatory components for rebuilding structural neural architecture.
The ultimate downstream consequence of this complex biochemical cascade is rapid, profound synaptogenesis TRD. Within 24 hours of a single subanesthetic administration, atrophied dendritic spines are physically restored, functional synaptic connections are re-established, and the overall micro-structural integrity of the prefrontal cortex is systematically elevated. This structural rewiring directly correlates with a profound down-regulation of the Default Mode Network (DMN), the neural highway responsible for maladaptive, self-referential depressive rumination.
Defining the Critical Window of Structural Malleability
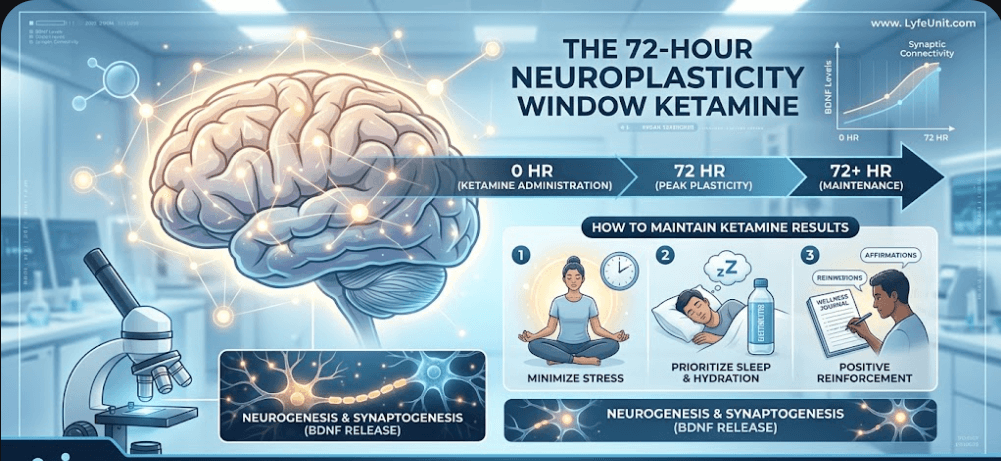
The intense structural transformation driven by synaptogenesis and dendritic remodeling creates a highly distinct, time-delimited state of neural hyper-plasticity. This biological window represents an epoch where the brain transitions from a state of calcified, rigid pathology into a highly malleable, adaptive medium—metaphorically transforming from hard clay into soft, impressionable wax. Clinical evaluations indicate that this hyper-plastic state peaks between 24 and 72 hours post-infusion, before slowly reverting to baseline homeostatic regulation.
Understanding the exact mechanics of this timeframe is crucial for long-term patient care. For a comprehensive breakdown of the structural changes during this phase, clinicians should review the data on the 72-hour neuroplasticity window after ketamine results. The primary clinical challenge is that neuroplasticity itself is entirely agnostic to behavioral direction. A highly plastic brain is fundamentally a highly sensitive brain; it will eagerly absorb, encode, and structurally reinforce whatever environmental inputs, cognitive patterns, and emotional stimuli it is subjected to during those critical 72 hours.
If a patient returns immediately to a high-stress, emotionally volatile, or deeply unsupportive environment following an infusion, the hyper-plastic brain will structurally consolidate those negative inputs, potentially accelerating a relapse into depressive pathology. Conversely, if systematic, therapeutic, and neuro-biologically supportive interventions are introduced while the mTOR pathway remains upregulated, the brain will preferentially stabilize healthy, adaptive, and resilient neural networks.
The Post-Ketamine Integration Protocol: A Three-Phase Framework
To successfully harness this biological opportunity, clinical practices must implement a rigorous, phase-specific post-ketamine integration protocol. This framework divides the 72-hour hyper-plastic window into actionable, strategic phases engineered to optimize synaptogenesis and maximize long-term therapeutic durability.
Phase 1: The Sensory Buffer and Acute Inward Focus (Hours 0 to 4)
The initial hours immediately following ketamine administration must be fiercely protected from external cognitive and sensory stimulation. Because the acute downregulation of the Default Mode Network leaves the patient highly sensitive to environmental inputs, the primary objective of this phase is metabolic and emotional stabilization. Protocols should mandate:
- Complete Digital Fasting: Patients must strictly avoid all smartphones, social media platforms, news media, and high-velocity digital communications. The algorithmic design of modern digital media exploits dopamine signaling pathways and can induce rapid cognitive fatigue in a hyper-plastic brain.
- Low-Stimulus Environments: Transition the patient to a dim, quiet space with minimal acoustic or visual variance. The utilization of non-lyrical, ambient music is highly recommended to encourage soft emotional processing without activating complex language centers.
- Somatic Stabilization: Prioritize somatic grounding techniques, such as breathwork and soft mindful awareness, to help the patient integrate the deep dissociative or mystical experiences often encountered during the session.
Phase 2: Cognitive Reconstruction and Targeted Psychotherapy (Hours 4 to 48)
This phase represents the clinical sweet spot for proactive psychological restructuring. Because the structural barriers of the ego are temporarily lowered, and the physical density of dendritic spines is actively increasing, the patient can engage with deep-seated traumatic material, maladaptive schemas, and negative self-talk without triggering a defensive amygdala response. The core interventions during this phase include:
- Ketamine-Assisted Psychotherapy (KAP): Schedule a dedicated integration therapy session within this 24-hour window. Utilize evidence-based modalities such as Acceptance and Commitment Therapy (ACT), Cognitive Behavioral Therapy (CBT), or Internal Family Systems (IFS).
- Narrative Reshaping and Journaling: Instruct the patient to engage in structured, free-form writing focused on processing insights gained during the session. This physically encodes cognitive realignments into newly forming neural pathways.
- Reframing Core Beliefs: Actively challenge long-standing depressive cognitive structures. The heightened plastic state allows for the rapid acquisition of new perspective frames that would typically take months to establish via standard talk therapy alone.
Phase 3: Behavioral Consolidation and Somatic Tracking (Hours 48 to 72)
The final phase of the acute window focuses on translating cognitive insights into permanent behavioral patterns. To ensure that newly formed synapses undergo long-term potentiation rather than metabolic pruning, patients must engage in specific physiological and behavioral actions:
- Sleep Architecture Optimization: Ensure the patient obtains 8 to 9 hours of uninterrupted sleep. Slow-wave sleep and rapid eye movement (REM) cycles are biologically mandatory for the physical consolidation of new synaptic connections and the stabilization of memory pathways.
- High-Intent Positive Habit Initiation: Introduce micro-habits during this phase, such as a 20-minute walk in nature, introductory mindfulness meditation, or structured physical exercise. The hyper-plastic brain will acquire these positive routines with significantly less friction than a typical depressive brain.
- Targeted Nutritional Support: Supply the metabolic building blocks required for rapid synaptogenesis. Protocols should emphasize an anti-inflammatory diet rich in Omega-3 fatty acids (specifically DHA and EPA), magnesium L-threonate, and polyphenols, which actively support and sustain endogenous BDNF synthesis.
Geo-Strategic Dynamics in Modern Interventional Psychiatry
From a macro geo-spatial perspective, the delivery model for interventional psychiatry is undergoing a significant transformation. Historically localized entirely within high-density academic medical centers, the availability of ketamine therapeutics has rapidly expanded into a decentralized ecosystem encompassing dedicated regional IV infusion clinics, hybrid psychiatric practices, and specialized at-home tele-health integration platforms. This spatial redistribution has drastically lowered geographic barriers to care, offering unprecedented access to individuals suffering from treatment-resistant conditions across diverse socio-economic corridors.
However, this rapid decentralization presents a distinct clinical continuity challenge. When a patient transitions between an isolated clinical infusion environment and their home setting, a critical “integration gap” frequently emerges. To close this gap, forward-thinking medical organizations are developing regional healthcare networks that link primary administration sites directly with local certified integration therapists, somatic coaches, and behavioral specialists. Managing this geographic and clinical continuity ensures that regardless of where the physical medicine is administered, the vital 72-hour window of structural neuroplasticity is seamlessly captured and optimized within a localized, supportive ecosystem.
Mitigating Plasticity Blockers and Confounding Variables
An exceptionally designed integration protocol is only as effective as its defensive measures. Clinicians must meticulously evaluate and eliminate a wide array of confounding variables and pharmacological agents that actively blunt, disrupt, or completely neutralize ketamine-induced neuroplasticity. Failure to manage these counter-indicators can result in complete failure of synaptogenesis.
Chief among these biological obstacles is the concurrent use of high-dose benzodiazepines. Medications such as alprazolam, clonazepam, and diazepam function as potent positive allosteric modulators of GABA-A receptors. By artificially amplifying inhibitory GABAergic tone, benzodiazepines directly counteract the upstream glutamate surge required to initiate AMPA receptor activation and subsequent BDNF exocytosis. Consequently, clinical protocols should strongly advocate for the strategic, medically supervised tapering or temporary suspension of benzodiazepines for at least 24 hours prior to and 48 hours following ketamine administration.
Furthermore, the consumption of ethanol within the 72-hour window is strictly contraindicated. Alcohol introduces severe neurotoxic stress, destabilizes sleep architecture, and directly downregulates the expression of the mTORC1 pathway, actively dismantling newly formed dendritic connections. Similarly, exposure to high-cortisol environments—such as hostile workplace dynamics or severe interpersonal conflict—must be systematically minimized, as sustained glucocorticoid signaling directly induces dendritic spine pruning, neutralizing the structural gains achieved during the treatment cycle.
Conclusion: Turning Biological Potential into Lasting Recovery
Subanesthetic ketamine therapy represents one of the most significant advancements in the history of interventional psychiatry, providing a rapid lifeline to individuals trapped in the debilitating architecture of Treatment-Resistant Depression. However, the true medical breakthrough is realized only when we treat ketamine not as a passive cure, but as a profound biological catalyst. The ultimate durability of the antidepressant response does not depend solely on the chemical compound itself, but on the systematic behavioral, environmental, and therapeutic protocols deployed while the brain remains in its uniquely malleable state.
By enforcing a structured, multi-phase post-ketamine integration protocol, medical providers and patients can consciously direct the course of synaptogenesis, building resilient neural networks that insulate the mind against future depressive relapse. The biological doorway to profound mental health recovery is opened by the medicine; walking through it permanently requires a precise, structured, and uncompromised clinical strategy.