Ketamine Effectiveness in the Management of Chronic Neuropathic Pain: A Clinical Deep-Dive
Living with chronic neuropathic pain is a bit like having a broken car alarm wired directly to your brain stem. It’s loud, it’s exhausting, it goes off at 3:00 AM for no reason, and kicking the dashboard (or downing traditional painkillers) rarely makes it stop. When standard pharmacological agents like gabapentinoids, tricyclic antidepressants, and traditional opioids fail to yield comfort, clinical focus shifts to deep-tier neurochemical interventions. This is where evaluating ketamine effectiveness in the management of chronic neuropathic pain transitions from an experimental concept into a critical frontline alternative.

The Molecular Mechanics: Why Nerve Pain Resists Normal Meds
To appreciate why ketamine works when traditional pain regimens crash and burn, we have to look at how chronic nerve pain alters your spinal real estate. Neuropathic pain—whether triggered by diabetic neuropathy, phantom limb syndrome, or trauma—is driven by a pathological phenomenon known as central sensitization. Think of it as your spinal cord setting its sensitivity dial to an absolute maximum.
When peripheral nerves continuously fire distress signals, they cause an over-accumulation of glutamate in the central nervous system. This excess glutamate continuously bombards the N-methyl-D-aspartate (NMDA) receptors. Once these NMDA receptors are chronically stuck in an “on” position, they trigger an escalated pain cycle often called “spinal wind-up.” At this stage, standard pain medications are effectively trying to lower the volume on a speaker system whose internal amplifiers have already melted down.
Enter NMDA Receptor Antagonism
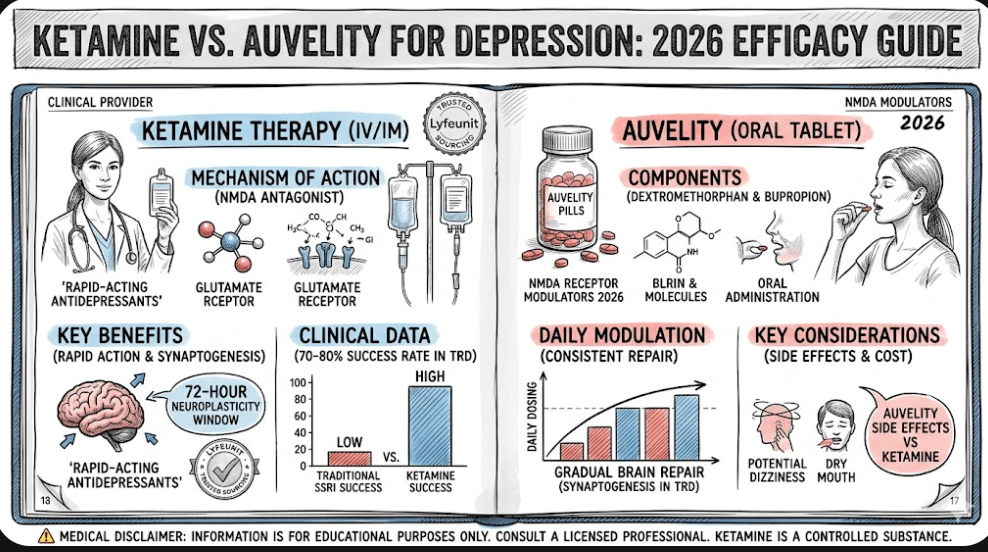
Ketamine is structurally unique because it behaves as a potent, non-competitive NMDA receptor antagonist. Instead of gently asking the nerve pathways to calm down, ketamine molecules bind deep inside the pore of the open NMDA receptor channel, actively cutting off the runaway electric currents. By temporarily silencing this overstimulated channel, ketamine interrupts the chronic feedback loop, stabilizing the hyperactive pathways and allowing the central nervous system to reset its baseline baseline sensitivity.
Quantifying Clinical Reality: What the Data Shows
Is ketamine a permanent cure? Let’s keep it strictly factual: No. But its clinical efficacy in breaking treatment-resistant cycles is well documented. Formal research synthesis indicates that sub-anesthetic, low-dose intravenous ketamine infusions deliver significant short-term analgesic benefits to patients suffering from severe refractory neuropathic syndromes.
According to comprehensive consensus guidelines established by the American Society of Regional Anesthesia and Pain Medicine (ASRA), the degree and longevity of pain relief are directly tied to the infusion profile. While basic 40-minute outpatient infusions show strong transient results, intensive, multi-day sub-anesthetic titration protocols provide cumulative analgesic effects that routinely persist for several weeks or even months.
| Administration Route | Average Bioavailability | Typical Relief Duration | Primary Clinical Role |
|---|---|---|---|
| Intravenous (IV) Infusion | 100% | 4 to 12 Weeks | Acute cycle breaking & profound baseline reset |
| Intranasal (Esketamine) | ~45% – 50% | Variable (Dose-Dependent) | Maintenance of therapeutic effect & psychiatric stabilization |
| Oral Formulations | 16% – 24% | Transient (Requires daily dosing) | At-home symptom management and baseline support |
Maximizing the Analytical Benefit: Overlapping Ecosystems
What makes ketamine uniquely fascinating to modern medicine is its dual-action profile. Chronic physical pain rarely travels alone; it almost always brings a heavy mental health tax, frequently presenting alongside severe treatment-resistant mood disturbances. When managing complex systemic cases, clinicians often look closely at how these neuropathic interventions interact with conditions like bipolar phenotypes, capitalizing on overlapping therapeutic properties to treat the whole person rather than just an isolated nerve circuit.
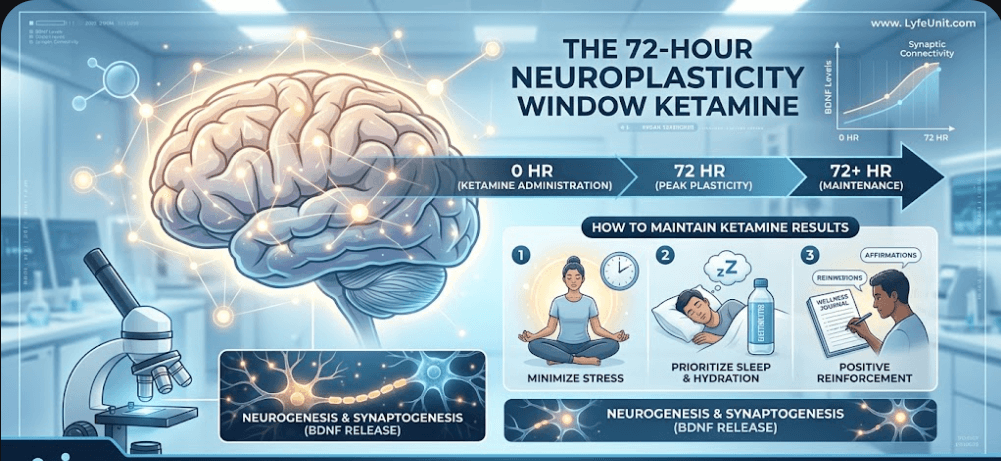
Furthermore, the physical relief observed in managing chronic neuropathic pain isn’t just about blocking a receptor for a few hours. The chemical clearance of the NMDA channel initiates a profound down-stream cellular cascade. As the nerve tissue catches its breath, the brain triggers a massive release of Brain-Derived Neurotrophic Factor (BDNF). This initiates a highly sensitive, crucial 72-hour neuroplasticity window after ketamine, giving the brain and spinal cord a temporary, structural window to actively re-forge damaged pathways and build healthier neural connections.
Optimizing Your Maintenance Strategy
While continuous in-clinic IV therapy remains the heavy machinery for breaking acute nerve pain loops, sustained care requires manageable, regulated maintenance alternatives. For patients seeking an FDA-approved, highly monitored delivery mechanism to sustain neural stability between intensive clinical blocks, options like the Spravato nasal system offer a reliable pathway forward.
Alternative Options and Co-Administrations
Because ketamine has a complex pharmacological profile, researchers are consistently looking for synergistic partners to extend its pain-killing lifespan while minimizing systemic side effects. Recent clinical data published via the Oxford Academic Pain Medicine Journal highlights that co-administering sub-anesthetic ketamine alongside membrane-stabilizing local anesthetics, such as intravenous lidocaine, often yields a potent synergistic effect, lowering pain scores far more efficiently than running either compound entirely on its own.
This multi-modal philosophy ensures that the central nervous system gets hit from multiple operational angles: ketamine halts the NMDA glutamate rush, while lidocaine systematically calms hyper-reactive, voltage-gated sodium channels. The result? A more complete silencing of ectopic nerve discharges and an extended operational window of relief for the patient.
When planning your complete treatment layout, it’s also worth discussing how these changes impact concurrent psychiatric landscapes. For instance, understanding the delicate adjustments required when introducing advanced NMDA modulators alongside ongoing treatments like ketamine for bipolar depression ensures that both your neurological pain metrics and emotional baselines remain safely aligned throughout the care cycle.
We wouldn’t be very good experts if we only talked about the sunshine and rainbows. Ketamine is a powerful dissociative anesthetic, and it brings some distinct, albeit temporary, eccentricities to the table during administration. During an infusion, you aren’t exactly going to be in shape to balance a checkbook or operate heavy machinery.
Common, acute side effects during treatment include:
- Dissociation: A distinct sensation of feeling detached from your physical body or immediate environment. (Many patients describe this as floating through a warm, slightly surreal landscape).
- Transient Hemodynamic Shifts: Temporary elevations in systemic blood pressure and heart rate that require active clinical monitoring.
- Psychomimetic Effects: Mild visual distortions or vivid dreams that typically fade rapidly once the active chemical infusion ceases.
When managed under strict, expert medical supervision within an accredited facility, these risks are heavily mitigated, leaving behind a highly tolerable and profoundly transformative clinical alternative for those who feel they have completely run out of options.
Frequently Asked Questions (FAQ)
1. What is the primary mechanism behind ketamine effectiveness in the management of chronic neuropathic pain?
Ketamine acts principally as a non-competitive antagonist of the N-methyl-D-aspartate (NMDA) receptor. By intercepting overstimulated glutamate signals, it shuts down central sensitization (“spinal wind-up”) and downregulates the hyperactive pathways transmitting persistent nerve pain.
2. How long does the pain relief from an intravenous ketamine infusion typically last for nerve damage?
Clinical evidence indicates that while immediate short-term analgesia is highly common, sustained therapeutic pain relief typically spans from 4 to 11 weeks, with some multi-day continuous titration protocols extending relief up to 3 months.
3. Can nasal or oral ketamine formulations match the effectiveness of IV infusions for chronic nerve conditions?
Intravenous (IV) delivery remains the gold standard for exact dosing and complete systemic bioavailability. However, targeted clinical interventions using managed options like Spravato esketamine nasal spray or carefully titrated oral doses serve as vital maintenance therapies to prolong the relief window without continuous hospital stays.