The Transformative Power of Ketamine Therapy | Mental Health Breakthrough
Quick Summary: What You Need to Know
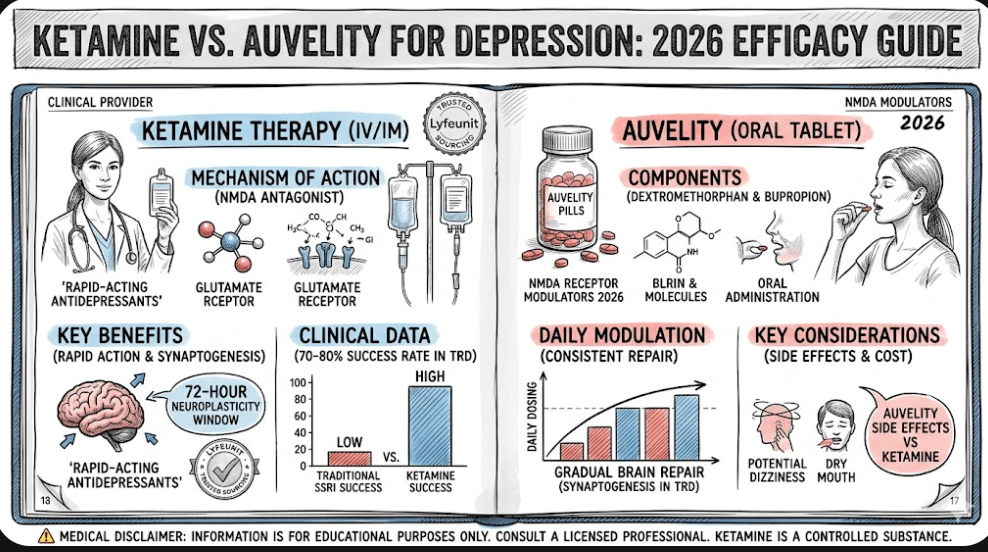
The transformative power of ketamine therapy lies in its ability to instantly bypass traditional monoaminergic pathways and trigger rapid structural neuroplasticity. While standard SSRIs require weeks to alter receptor density, sub-anesthetic ketamine acts within hours as an NMDA receptor antagonist, causing a glutamate storm that repairs atrophied dendritic spines. To transform a transient biochemical reset into permanent clinical remission, patients must explicitly exploit the temporary 72-hour cellular window with proactive psychological integration, monitored titration, and structured maintenance strategies.
If you have spent years cycling through standard psychiatric medications, your relationship with the pharmaceutical industry probably feels like a bad series of unreciprocated text messages. You wait six weeks for an SSRI to kick in, only to realize the primary biological shift it achieved was giving you dry mouth and the emotional range of a garden paver. When the conventional system defaults to therapeutic stagnation, understanding the transformative power of ketamine therapy | mental health breakthrough transitions from an intriguing academic curiosity into an absolute clinical necessity.
For decades, psychiatry operated under the rigid assumption that mood disorders were simply a software shortage—not enough serotonin or norepinephrine floating around in the synaptic cleft. We now know that chronic stress, trauma, and unyielding neuropathic distress actually cause physical hardware damage: specifically, the structural atrophy of dendritic connections within the prefrontal cortex. Ketamine is fundamentally changing this paradigm by acting as an immediate hardware reboot rather than a slow, system-taxing software patch.
The Molecular Mechanics of a Clinical Disruption
To grasp why this molecule has triggered an international paradigm shift, we must look directly at its competitive cellular target. Ketamine operates principally as a high-affinity, non-competitive antagonist at the N-methyl-D-aspartate (NMDA) receptor channel. By transiently blocking these pathways on gamma-aminobutyric acid (GABA)-ergic interneurons, ketamine disinhibits the system, causing an immediate, controlled surge of extra-cellular glutamate.
This localized glutamate rush targets adjacent alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors. The subsequent depolarization triggers a massive intracellular signaling cascade, culminating in the rapid upregulation of Brain-Derived Neurotrophic Factor (BDNF) and the downstream activation of the mammalian target of rapamycin (mTOR) pathway. In plain English: it’s an organic fertilizer blast for a withered neural landscape.
This cellular remodeling explains why ketamine could save your life during an acute psychiatric crisis. Traditional antidepressants attempt to rebuild the bridge while cars are actively falling off it; ketamine drops a structural steel support beam into place within hours, offering rapid anti-suicidal properties that have completely redefined emergency psychiatric triage across the globe.
One of the most frequent hurdles for incoming patients is separating the medicinal utility of the substance from its historic counter-cultural reputation. It is common to wonder: does ketamine therapy get you high, or is there a functional clinical distinction between recreational dissociation and sub-anesthetic neuro-restoration?
During a clinical infusion, patients routinely experience a dose-dependent state of light dissociative anesthesia. You might feel as if your mind has temporarily detached from your physical coordinates, or find yourself viewing your life’s narrative arcs with the objective detachment of a nature documentary narrator. This isn’t an accidental side effect; it is a critical component of the transformative power of ketamine therapy | mental health breakthrough. By decoupling the emotional alarm systems of the amygdala from your core autobiographical memories, ketamine allows patients to look directly at deeply rooted trauma without re-traumatizing the nervous system.
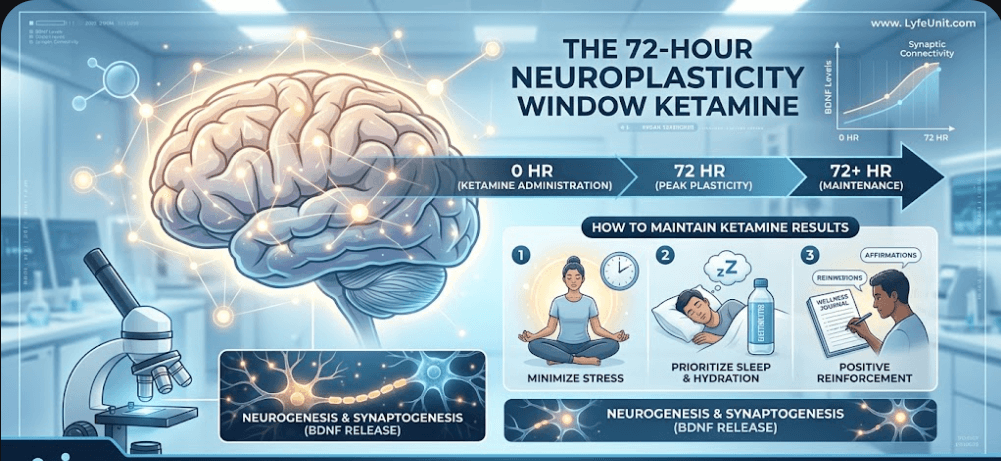
However, the magic isn’t just in the psychological journey itself. The long-term clinical utility is driven entirely by what happens when you land. The immediate post-infusion chemical cascade kicks open a hyper-receptive 72-hour neuroplasticity window after ketamine results. During this brief, critical timeframe, your brain is structurally malleable—behaving less like cured concrete and more like fresh clay. If you leave the clinic and immediately return to doom-scrolling or toxic environments, you run the risk of inadvertently hardening those same maladaptive pathways right back into place.
Maximizing Long-Term Remission: Integration and Timing
Because the brain enters this ultra-malleable phase, structural success is heavily reliant on a structured behavioral protocol. Knowing exactly ketamine integration what to do after session completion determines whether your breakthrough remains a fleeting weekend vacation or transforms into enduring neural freedom. Integration work—whether through specialized somatic therapy, targeted journaling, or specific mindfulness routines—is what explicitly translates temporary chemical space into permanent behavioral habits.
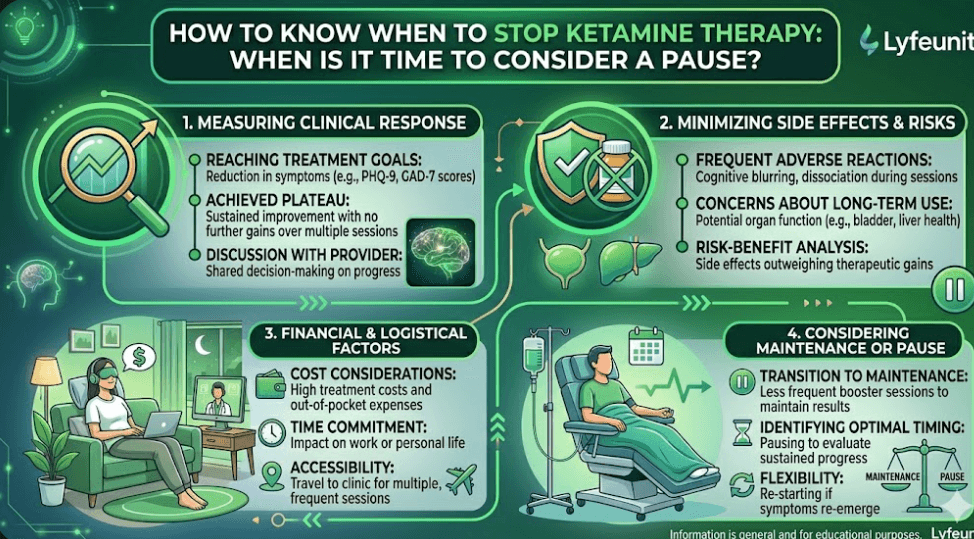
Further, because this intervention operates on a cumulative dosing logic, clinical oversight must remain highly personalized. Patients shouldn’t look at this as an open-ended, infinite loop of dependency. Developing a clear, structured blueprint with your medical provider on how to know when to stop ketamine therapy guarantees that you successfully transition from an intensive induction schedule to an adaptive, long-interval maintenance baseline once structural stabilization is achieved.
The Broad Spectrum of Care: From Mood to Neuropathy
While the broader public narrative focuses heavily on unipolar major depression, clinical protocols have proven remarkably agile at addressing more intricate, dual-diagnosis presentations. For instance, utilizing tailored, titrated protocols of ketamine for bipolar depression has shown incredible efficacy in rapidly lifting individuals out of profound depressive troughs without inadvertently inducing hyper-reactive manic switching—a notorious complication long associated with traditional monoamine-based agents.
Moreover, the clinical utility extends deep into severe somatosensory conditions. In settings like specialized pain clinics, utilizing a targeted ketamine vial nerve pain relief Florida protocol allows interventional specialists to run longer, higher-dose infusions designed to forcefully reset the chronic spinal wind-up loops responsible for severe treatment-resistant neuropathy and complex regional pain syndromes (CRPS).
| Clinical Presentation | Primary Neurological Target | Typical Infusion Protocol | Expected Relief Mechanism |
|---|---|---|---|
| Treatment-Resistant Depression | Prefrontal Synaptogenesis | 0.5 mg/kg over 40 minutes | Rapid restoration of dendritic spines; BDNF surge |
| Bipolar Depressive Troughs | Glutamate Homeostasis | Sub-anesthetic slow titration | Rapid mood elevation without manic switching |
| Chronic Neuropathic Pain | Spinal NMDA Over-Sensitization | 1.0 – 2.0 mg/kg over 2-4 hours | Disruption of central spinal wind-up loops |
The practical reality of accessing this breakthrough requires a modern understanding of medical logistics, supply chains, and evolving insurance standardizations. The clinical space has faced notable structural volatility recently; tracking developments via a dedicated compounded ketamine guide 2026 ketamine shortage highlights how institutional supply chain strains have forced leading clinics to adapt their compounding methodologies to safeguard patient care continuity.
Simultaneously, financial accessibility is undergoing a dramatic structural evolution. Reviewing the latest legal and institutional updates on does insurance cover ketamine therapy for depression in 2026 shows that while generic IV infusions often remain an out-of-pocket or superbill-driven cost, commercial insurance payers have increasingly standardized robust prior-authorization frameworks for targeted, FDA-approved delivery systems to manage treatment-resistant depressive phenotypes.
Spravato Esketamine 56mg Nasal Spray Dose Kit
The premium, FDA-approved intranasal delivery infrastructure designed explicitly for targeted treatment-resistant depression protocols under clinical supervision.Explore Spravato Nasal Kit Options
Rotexmedica Ketamine Injection Infrastructure
Premium-grade pharmaceutical preparation optimized for precise clinical titration, systemic bioavailability, and profound NMDA-receptor blockade protocols. View Rotexmedica Pharmaceutical Specifications
Why the Speed of Action Matters Intracellularly
The final pillar of understanding why ketamine is such a powerful antidepressant relates directly to its temporal footprint. When a patient is locked in an intense, life-threatening depressive paralysis, telling them to wait months for a traditional pill to modify gene expression is an unacceptable clinical risk.
By forcing an immediate, localized efflux of acetylcholine and downstream glutamate, ketamine functions like a molecular jumper cable on a flat battery. Clinical trial data aggregated across major psychiatric institutions shows that a single sub-anesthetic administration can significantly clear suicidal ideation indices within four hours, mapping a trajectory of symptom reduction that correlates perfectly with the physical remodeling of mood-regulating circuits in the brain. According to critical peer-reviewed insights published in PubMed Central (PMC) Lit Reviews, this rapid turnaround solidifies NMDA modulation as the most parsimonious path to restoring underlying deficits in molecular neuroplasticity.
To further validate these mechanics, comprehensive consensus statements compiled by the Translational Psychiatry Journal confirm that NMDA-receptor inhibition rapidly increases the brain’s baseline receptiveness to learning entirely new emotional responses. Additionally, long-term safety tracking published across the MDPI Medical Review Series demonstrates that structured, intermittent low-dose maintenance cycles effectively prevent the structural dendritic regression commonly driven by chronic, unmanaged environmental stress.
Frequently Asked Questions (FAQ)
1. Why is ketamine therapy considered a major mental health breakthrough compared to SSRIs?
Traditional SSRIs function by slowly increasing monoamine neurotransmitter levels in the synaptic cleft, a process that can take weeks to yield structural changes. In contrast, ketamine bypasses this system entirely by acting as a non-competitive NMDA receptor antagonist. This triggers an immediate surge of glutamate, rapidly accelerating synaptogenesis and restoring neural connectivity within hours.
2. How does the neuroplasticity window maximize the transformative power of ketamine therapy?
Ketamine initiates a critical, transient neuroplastic state driven by the up-regulation of Brain-Derived Neurotrophic Factor (BDNF) and the downstream activation of the mTOR pathway. This state lasts approximately 72 hours post-infusion, providing a golden window where the brain is highly adaptable, allowing therapeutic interventions and positive behavioral cognitive changes to integrate permanently.
3. Does insurance cover ketamine infusions for psychiatric conditions currently?
Coverage for off-label generic intravenous ketamine infusions remains variable among commercial insurers. However, FDA-approved intranasal formulations like Spravato esketamine are widely covered by major medical insurance policies for treatment-resistant depression (TRD) and major depressive disorder with acute suicidal ideation, provided specific clinical criteria are documented.
Lyfeunit BueSky Socials