Why Ketamine Could Save Your Life: The Rapid-Acting Neuroplasticity Breakthrough
By: Lyfe Unit Editorial Team
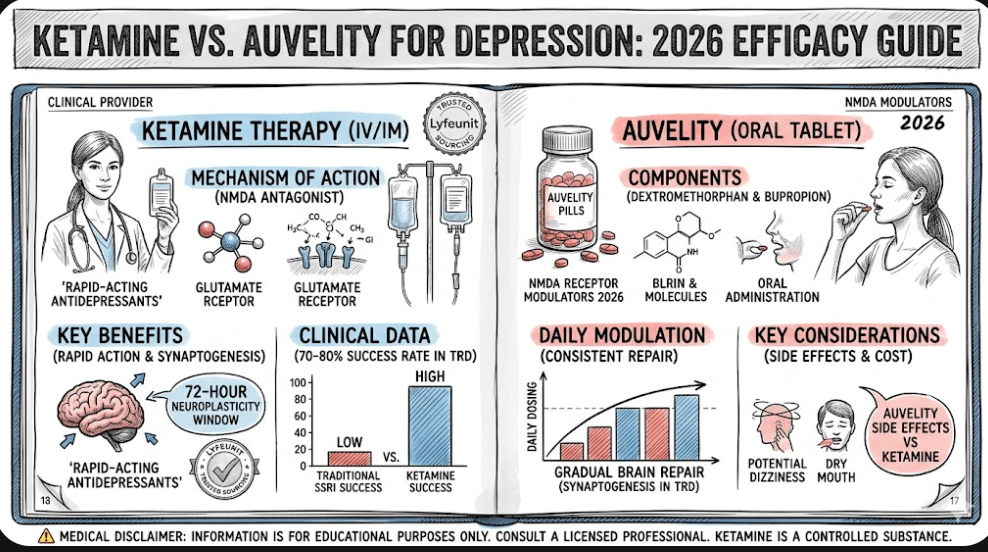
What you need to know: Traditional antidepressants take 4 to 6 weeks to disrupt severe mental health crises, leaving a dangerous therapeutic gap. Modern clinical evidence reveals that sub-anesthetic doses of ketamine trigger structural neuroplasticity and evacuate G-proteins from lipid rafts within 15 minutes to 4 hours. This fast-acting biochemistry halts active suicidal ideation and reverses treatment-resistant depression independently of classic NMDA-receptor pathways. In short: Why ketamine could save your life comes down to speed, molecular remodeling, and its unique ability to restore broken neurological communication channels when traditional SSRIs fail completely.
For decades, psychiatric medicine has operated under an agonizingly slow paradigm. If you suffer from severe clinical depression, the standard response has been a prescription for Selective Serotonin Reuptake Inhibitors (SSRIs). Then comes the wait. Four weeks, six weeks, perhaps months of chemical trial-and-error while navigating a gauntlet of emotional numbness and systemic side effects.
When you are stranded in the deep, dark trenches of a mental health crisis, six weeks is not just an inconvenient delay—it is an existential vulnerability. This is precisely why ketamine could save your life. As the only widely utilized psychotherapeutic substance with rapid-acting efficacy, ketamine is rewriting the rules of neurobiology, stepping in as a biological shield when traditional therapies fall short.

The Paradigm Shift: From Serotonin to Glutamate and Lipid Rafts
To understand why this compound is capturing the attention of geo-strategists in mental health care, we have to look past its historical reputation. Long classified simply as a veterinary anesthetic or a counter-culture hallucinogen, ketamine is now recognized as a premier catalyst for neurological regeneration.
Unlike standard SSRIs that target the serotonin system, ketamine works directly on glutamate, the most abundant neurotransmitter in the mammalian central nervous system. Glutamate is the operational engine behind roughly 40% of all cellular connections (synapses) in the brain. It is the fundamental fuel for learning, memory formation, and executive cognitive function.
When an individual experiences chronic stress, trauma, or severe mood disorders, the brain suffers physical degradation. The delicate, branch-like structures on neurons called dendrites—which function as the communication highways between the prefrontal cortex and the hippocampus—begin to wither and atrophy. The brain loses its structural flexibility. It gets stuck in a toxic, repetitive loop of despair.
Ketamine radically alters this trajectory. By prompting an immediate surge in glutamate, it stimulates mammalian target of rapamycin (mTOR) pathways, rapidly generating new dendritic spines. This structural remodeling allows the brain to heal its physical architecture, bypassing the damaged pathways that lock a person into depressive cycles.
The 15-Minute Molecular Migration
Groundbreaking cellular research led by Dr. Mark Rasenick, a distinguished professor of physiology and psychiatry at the University of Illinois at Chicago College of Medicine, has unveiled an even deeper mechanism. For years, the scientific community believed ketamine’s therapeutic benefit was exclusively dependent on blocking N-methyl-D-aspartate (NMDA) receptors. Dr. Rasenick’s findings turned this assumption on its head.
In patients suffering from deep clinical depression, signaling molecules called G-proteins become physically trapped inside “lipid rafts”—dense, oily patches on the cell membrane. When stuck inside these rafts, G-proteins are held inactive, preventing them from producing cyclic AMP, a compound vital for clear neural signaling. This cellular traffic jam contributes directly to the pervasive sense of emotional numbness reported by patients.
While traditional SSRIs do gradually coax G-proteins out of these lipid rafts, the process takes days or weeks. When exposed to ketamine, however, the migration begins almost immediately. Within 15 minutes, G-proteins begin fleeing the lipid rafts, restoring cellular communication at breakneck speed. Even more profound: because these signaling molecules are incredibly slow to drift back into the lipid rafts, the antidepressant effects persist long after the drug’s brief six-hour half-life has cleared the body.
Maximizing the Meta-State:
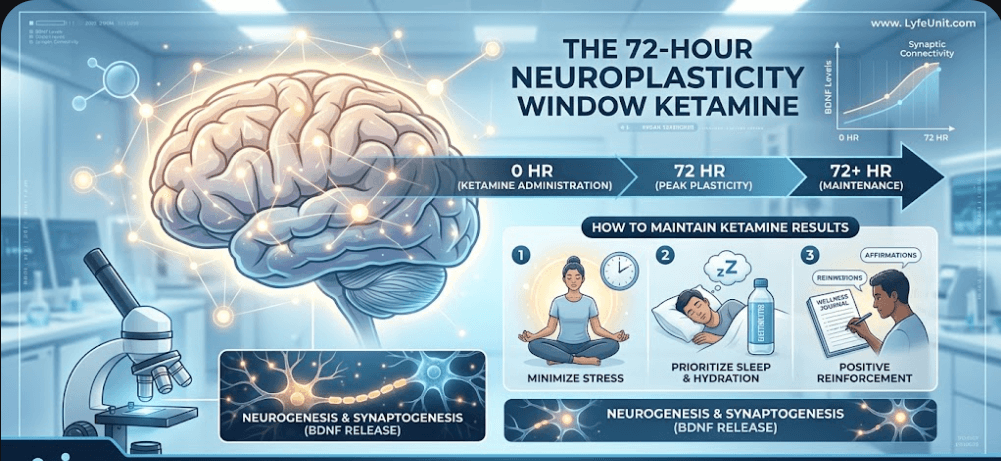
The swift relocation of G-proteins and the sudden burst of glutamate create a highly specialized neurological state. This phase is known clinically as a transient period of hyper-plasticity, where the brain becomes exceptionally malleable and receptive to new cognitive frameworks.
To convert this biological intervention into permanent mental wellness, patients must actively capitalize on the immediate post-infusion period. Understanding how to manage the critical 72-hour neuroplasticity window after ketamine results is vital. During this specific timeframe, behavioral modifications, therapeutic integration, and positive lifestyle inputs are effectively fast-tracked into the brain’s newly forming physical infrastructure, cementing long-term psychological resilience.
What the Evidence Says: A Comprehensive Data Review
To evaluate the comprehensive landscape of this treatment, a massive systematic analysis published in the British Journal of Psychiatry Open examined data across 83 peer-reviewed, published research papers. The scope of this meta-review was extensive, encompassing:
- 33 systematic reviews
- 29 randomized controlled trials (RCTs)
- 21 rigorous observational and open-label trials
The conclusions of this definitive data review were stark: the most robust, undeniable therapeutic efficacy for sub-anesthetic ketamine lies in its treatment of major depressive disorder (MDD) and complex mood cycling. For individuals navigating severe mood dysregulation, exploring specialized interventions like ketamine for bipolar depression offers a rapid, scientifically validated path away from treatment resistance.
Crucially, the review highlighted an extraordinary clinical phenomenon: ketamine reduces suicidal ideation to a significant degree, completely independent of its antidepressant effects.
“People have reviewed the effects on depression and bipolar disorder, but ketamine is beginning to be used for a wider range of psychiatric disorders,” notes Celia Morgan, a professor of Psychopharmacology at the University of Exeter. “It is a really interesting effect that when we parse out effects on depressive symptoms, there is still evidence of a reduction in suicide.”
An Emergency Shield Across Diagnostics | Why ketamine could save your life
In acute crisis scenarios, traditional medicine faces an operational roadblock. When an individual enters an emergency department experiencing acute suicidality, clinicians rarely have immediate access to a comprehensive psychiatric history. They may not know if they are treating underlying major depression, substance-induced psychoses, borderline personality traits, or co-occurring trauma.
Because ketamine’s anti-suicidal mechanism operates via global structural neuroplasticity and rapid G-protein clearance rather than standard diagnostic-specific monoamine adjustments, it works universally. This makes it an invaluable asset for crisis intervention.
A single clinical dose can cause active suicidal ideation to plummet within 1 to 4 hours, keeping those thoughts at bay for up to two weeks. This rapid mitigation provides critical emergency windows for stabilization, psychiatric assessment, and long-term care routing.
The Expanding Horizon: Anxiety, PTSD, and Behavioral Conditions
While mood disorders and acute crises remain the primary clinical targets, emerging clinical trials are exploring ketamine’s applications across a broader psychiatric spectrum. Early data indicates substantial efficacy in providing short-term relief from cravings and distressing physiological withdrawal symptoms in individuals struggling with severe substance use disorders.
Furthermore, pilot studies demonstrate immense promise for treating Post-Traumatic Stress Disorder (PTSD), obsessive-compulsive loops, and generalized anxiety states. By temporarily calming the overactive amygdala—the brain’s threat-detection center—ketamine allows patients to process traumatic memories or deeply ingrained behavioral compulsions without being overwhelmed by intense emotional terror.
Researchers are also eager to evaluate its efficacy for complex eating disorders, such as restrictive anorexia nervosa. Given the exceptionally high mortality rates associated with severe eating disorders, utilizing an intervention that rapidly disrupts rigid, destructive cognitive loops could prove transformative. While clinical recruitment within these vulnerable populations remains inherently complex, current global trials aim to unlock these precise therapeutic applications over the coming years.
Accessing the Breakthrough: Modern Delivery Mechanisms
As the clinical infrastructure expands globally, patient access has moved beyond traditional intravenous (IV) clinics into regulated, targeted outpatient administration options. For many seeking a structured, FDA-approved protocol that fits seamlessly into an ongoing psychiatric plan, intranasal delivery has emerged as an optimal choice.
Qualified healthcare providers frequently recommend specialized solutions such as the Spravato Esketamine 56mg Nasal Spray Dose Kit. Administered strictly under medical supervision, this targeted system provides rapid systemic absorption, offering a practical avenue for patients battling treatment-resistant depression to reclaim their neurological agency safely.
The Strategic Path Forward: Personalizing Psychedelic Medicine
Despite the overwhelming promise, experts emphasize that ketamine is not an magical, universal cure-all. It is a powerful biochemical tool. According to data compiled by the National Institutes of Health, approximately one-third of treatment-resistant patients may not show a significant response to standard ketamine protocols.
“It doesn’t work for everyone,” Professor Morgan cautions. “Because of the strong promise of this new treatment approach, not responding can leave people feeling even more hopeless. If we can determine who it will and won’t work for beforehand, that will be incredibly useful.”
Modern psychopharmacology is moving swiftly toward identifying unique biomarkers—such as specific genetic variations or baseline neuroimaging profiles—to accurately predict patient response. Until those predictive frameworks are fully mature, the optimal strategy requires a multi-faceted approach: combining rapid-acting chemical delivery with robust, trauma-informed psychological integration.
By protecting the brain’s physical architecture, promoting rapid cellular communication, and offering an immediate bridge over acute crises, ketamine has firmly established itself as a cornerstone of modern neuro-stratigraphy. In the ongoing fight against severe mental health challenges, it stands out as a rapid-acting asset built to safeguard human life when every minute counts.
Frequently Asked Questions (FAQ)
How quickly does ketamine start working for depression?
Unlike traditional monoaminergic antidepressants (SSRIs/SNRIs) which typically require 4 to 6 weeks to show clinical benefits, sub-anesthetic ketamine works incredibly fast. Dr. Rasenick’s molecular research demonstrates that G-proteins begin moving out of lipid rafts within 15 minutes of administration. Patients frequently experience a significant reduction in depressive symptoms and a clearance of suicidal ideation within 1 to 4 hours post-treatment.
Does ketamine cure depression permanently?
No, ketamine is not a permanent one-time cure. A single sub-anesthetic clinical session typically provides rapid relief that lasts between one to two weeks. To achieve long-term, sustained remission, it is crucial to capitalize on the heightened neuroplastic window following treatment. Coupling the physiological effects with professional therapeutic integration, routine lifestyle changes, or maintenance protocols helps build permanent neural connections. For safety and clinical efficacy data on modern protocols, consult the comprehensive World Health Organization Medical Publications.
What is the difference between ketamine and Esketamine (Spravato)?
Standard ketamine is a racemic mixture containing two mirror-image molecules: R-ketamine and S-ketamine, typically delivered via intravenous (IV) infusion or intramuscular injection. Esketamine (Spravato) isolates the specific “S” enantiomer. It is FDA-approved specifically for treatment-resistant depression (TRD) and major depressive disorder with acute suicidal ideation, delivered via a regulated nasal spray device under direct in-office medical supervision.
How does ketamine rapidly stop suicidal thoughts?
Remarkably, clinical data shows that ketamine clears suicidal ideation independently of its general antidepressant effects. It achieves this by rapidly fixing damaged communication points (dendritic spines) in the prefrontal cortex and restoring healthy cell signaling. This fast action temporarily deactivates the brain’s acute distress networks across multiple diagnoses. For insights into active clinical trials investigating fast-acting psychiatric interventions, visit the official U.S. National Institutes of Health Clinical Trials Database.
Is ketamine treatment safe under medical supervision?
Yes, when administered at sub-anesthetic doses in a controlled clinical environment by qualified healthcare practitioners, ketamine maintains an excellent safety profile. The dose used for psychiatric indications is significantly lower than the amount used for surgical anesthesia. Transient side effects during the session can include mild dissociation, brief elevations in blood pressure, or temporary nausea, all of which typically resolve completely within 60 to 90 minutes.
Crisis Support Notice: If you or a loved one are experiencing an active mental health crisis, profound despair, or thoughts of self-harm, please connect with immediate assistance. Call or text 988 to reach the Suicide & Crisis Lifeline (in the US and Canada), or contact your local emergency services immediately. Help is available, and you do not have to carry this weight alone.